What Changed in Rectal MRI Staging: The 2026 ESGAR Update
ESGAR's first rectal MRI update since 2018. Part I covers primary staging and the changes that touch your report.
ESGAR updated its rectal cancer MRI guidelines for the first time since 2018. This is Part I, primary staging. Most of the old framework holds. A handful of changes touch your report, and those are worth knowing.
The process was solid. Twenty-six abdominal radiologists from eighteen countries, a formal RAND-UCLA consensus, 126 items scored, 96% consensus. Only five items fell short, and even those reached 77%. So this is broad agreement, not one group’s preference.
Here’s what actually changed, most consequential first.
The sigmoid take-off decides rectal versus sigmoid. The STO is the newer landmark. On a sagittal image, it’s the point where the sigmoid sweeps horizontally, away from the sacrum. On axial, where it turns ventrally. Lower tumor border at or below the STO is rectal. Above it, sigmoid. It’s moderately to well reproducible, with some interpretation pitfalls.
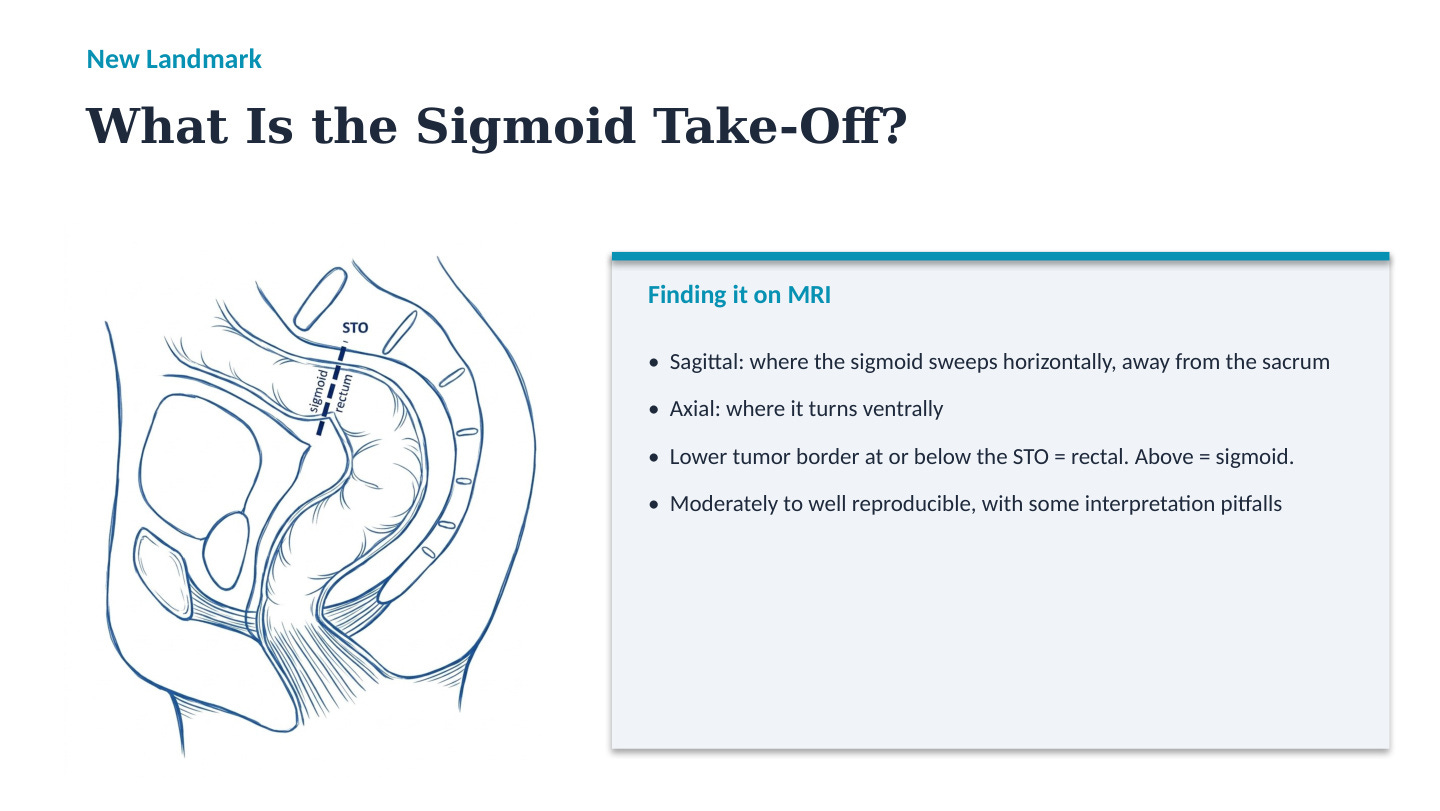
This isn’t cosmetic. The evidence says using the STO shifts treatment planning in 20 to 30% of cases compared to older landmarks. A tumor you’d have called rectal can now be staged and managed as sigmoid.
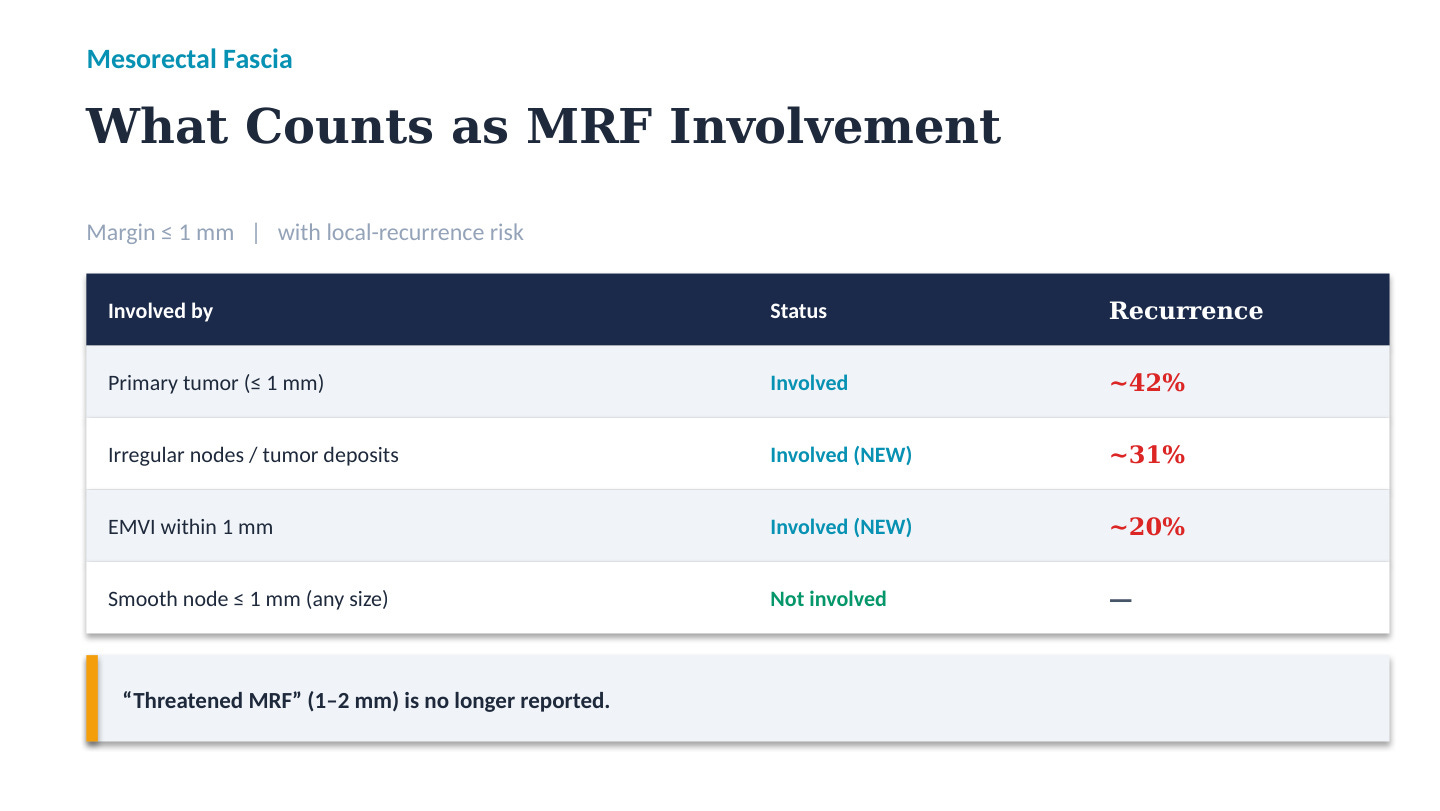
“Threatened MRF” is gone. The old 1 to 2 millimeter category caused confusion and the data didn’t support it. Stop reporting it. The 1 millimeter cutoff for involvement stays. What’s new is that EMVI and irregular nodes within 1 millimeter now count as MRF involvement, not just direct tumor extension. Recurrence risk backs it up: about 42% for direct invasion, 31% for irregular nodes, 20% for EMVI. The flip side, a smooth node within 1 millimeter, any size, is not involvement.
Nodes move to a patient-level call. This is the biggest shift in thinking. You still apply size and morphology to individual nodes, but then you fold in the other risk factors, higher cT, EMVI, more suspicious nodes, and report a confidence level: definitely cN0, possibly cN+, or definitely cN+. I think this is the honest move. MRI nodal staging was never precise. The guideline stops pretending and asks you to state how sure you are.
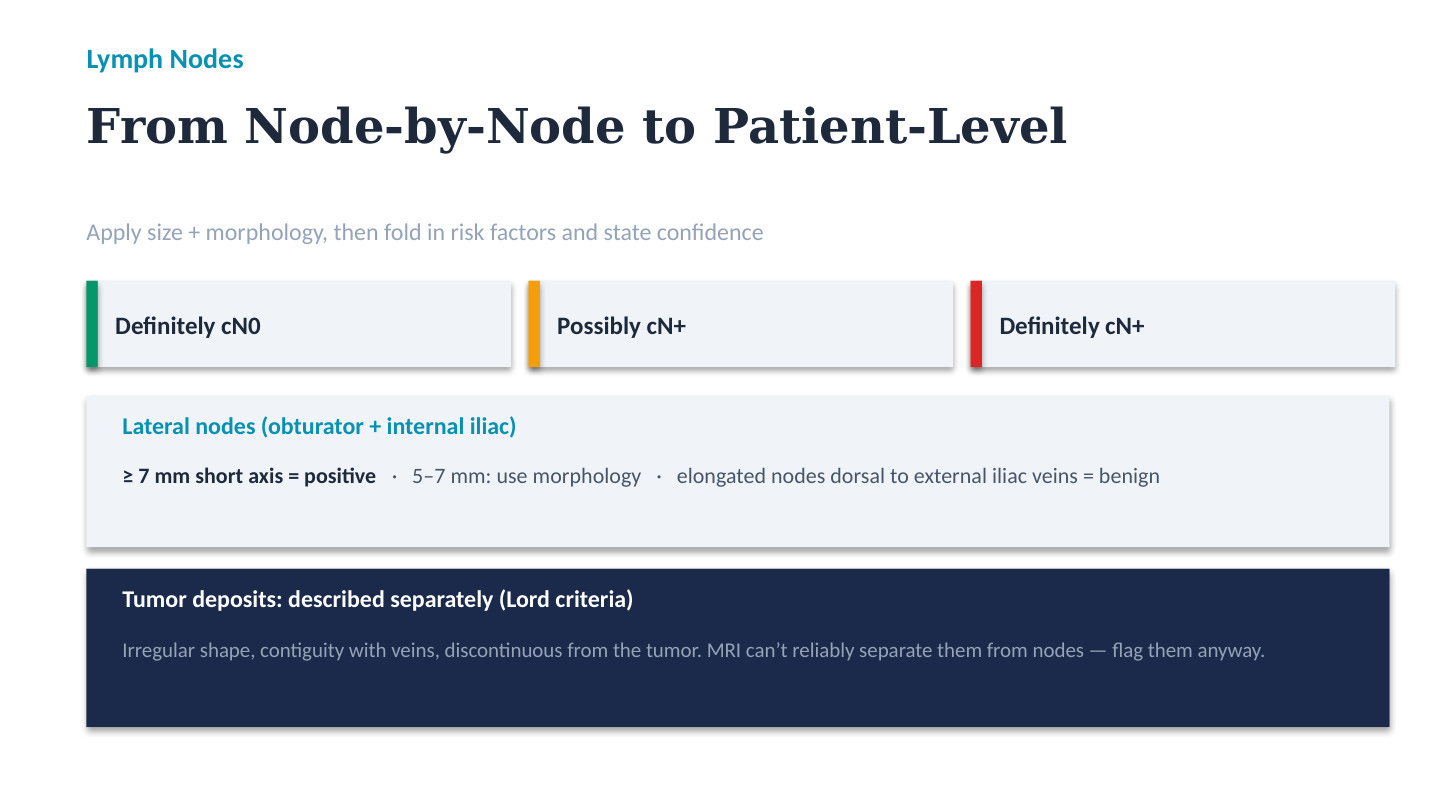
Lateral nodes finally get a threshold: 7 millimeters short axis for obturator and internal iliac. Between 5 and 7, use morphology. Elongated nodes just behind the external iliac veins are benign, so don’t flag those. Tumor deposits get a separate description using the Lord criteria, irregular shape, contiguity with veins, discontinuous from the tumor.
DWI and AI both get pulled back. DWI stays in the protocol but its role narrowed, read it with T2, use it to find nodes and small tumors, don’t use it for T-category, EMVI, MRF, or ADC-based staging. Radiomics and deep learning should not guide clinical decisions yet. Small studies, retrospective designs, not enough prospective validation.
What ties this together is a move away from rigid TNM toward risk-adaptive staging. More of the report is now a judgment under uncertainty, stated plainly, rather than a checkbox. That’s the part of the read where a second set of eyes that reasons with you actually helps. It’s why I built RadReason the way I did.
This was primary staging. Part II covers restaging and response after neoadjuvant treatment. That’s the next episode.
Watch the full episode: RadBrief EP02 on YouTube
Sources:
ESGAR Rectal Imaging Guideline Group. “MRI to guide clinical management of rectal cancer: updated consensus recommendations from ESGAR — PART I primary staging.” European Radiology 2026. DOI 10.1007/s00330-025-12274-w.
ESGAR Rectal Imaging Guideline Group. “PART II restaging and response evaluation.” European Radiology 2026. DOI 10.1007/s00330-025-12275-9.