What Changed in Rectal MRI Restaging: The 2026 ESGAR Update
Part II of the ESGAR update. Restaging after neoadjuvant treatment, rebuilt around organ preservation.
This is Part II of the ESGAR update, restaging after neoadjuvant treatment. The headline: restaging has been rebuilt around organ preservation. The question used to be “what stage is it now.” Now it’s “is this a complete responder who can keep their rectum.” That reframe drives the rest.
Same panel and process as Part I, 49 restaging items, 98% consensus. One item fell short at 73%, whether to use the same response criteria for solid and mucinous tumors.
Here’s what changed.
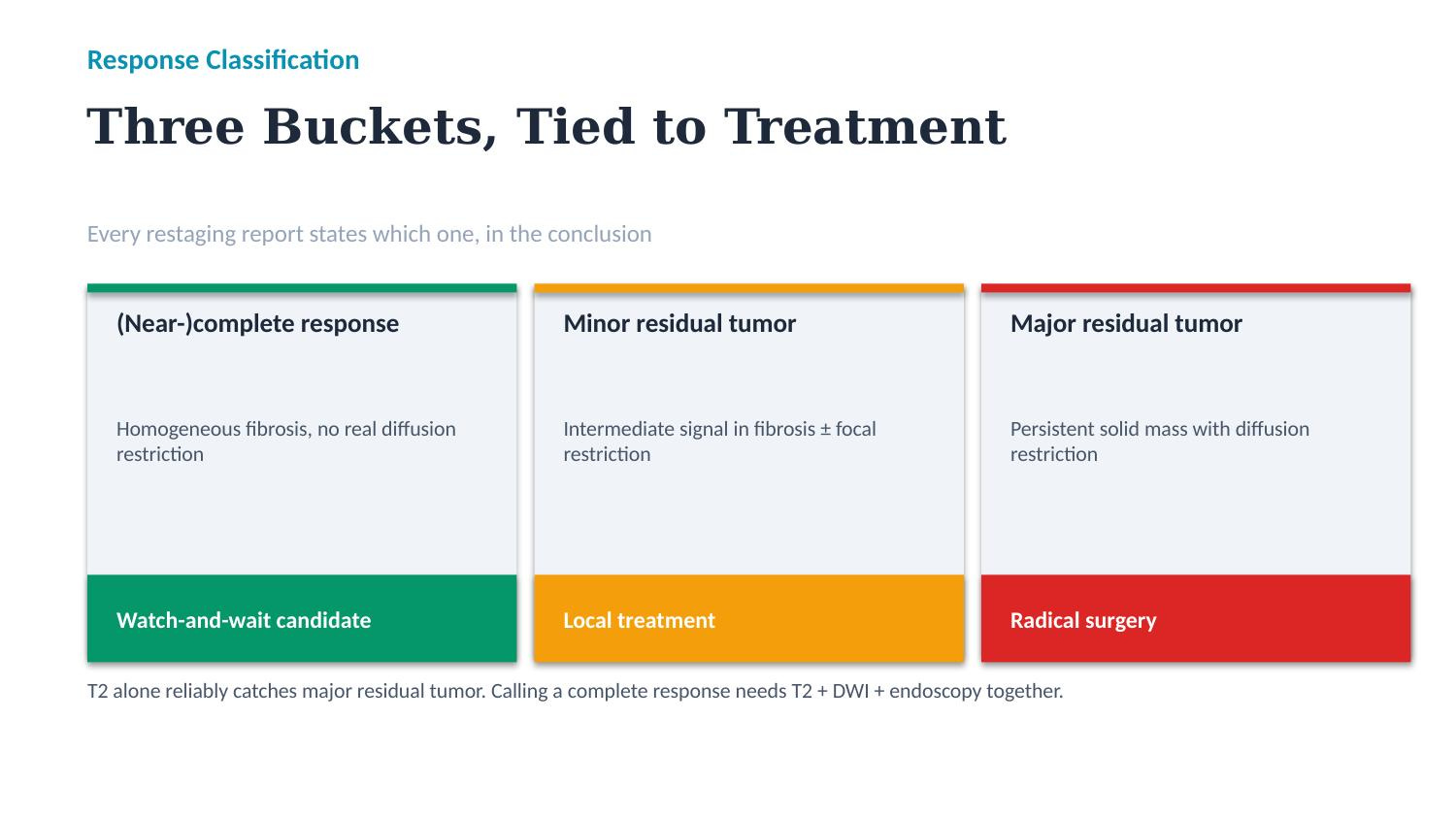
Every report needs a response classification. Three categories, each tied to a treatment path. Complete or near-complete response, homogeneous fibrosis with no real diffusion restriction, these are watch-and-wait candidates. Minor residual tumor, some intermediate signal in the fibrosis, possible local treatment. Major residual tumor, a persistent solid mass with restriction, radical surgery. Say which bucket in the conclusion. T2 alone reliably catches the major residual tumors, but calling a complete response needs T2, DWI, and endoscopy together.
Stop forcing a ycT in complete responders. In a suspected complete or near-complete response, don’t report a detailed ycT. It’s unreliable and a range like ycT0-3 just risks disqualifying someone from organ preservation. This is a change from 2018, which asked for a ycT in every case. When there is residual tumor, report ycT as a maximum estimate and measurements should encompass the whole fibrotic remnant of the tumor bed.
One US caveat. This is a European panel. In every US institution I’ve worked in, we don’t restage the primary tumor with a ycT at all, we just describe the response. Nodes we do restage. If that’s your practice, the panel’s point still holds, don’t put a confident T-category on fibrosis.
DWI is now mandatory for response assessment. It’s what separates residual tumor from complete response. Use it for one job in T-staging, ycT0 versus ycT-positive. Read DWI together with the ADC map and the shape of the signal, that’s how you filter T2 shine-through, susceptibility artifact, and inflammatory signal from ulcerated areas. Remember the MRI response lags the histologic response. Residual abnormalities can sit on the scan when there’s little or no viable tumor left, so in a borderline near-CR, a second look at short interval is reasonable. mrTRG gives a rough good-versus-poor read but can’t reliably call a complete response, so it’s not in the template.
MRF and EMVI get treatment-specific rules. If a fat plane reappears between tumor and fascia, call the margin cleared (ycMRF-negative). Stranding alone is equivocal. The 1 mm cutoff stays. One useful shift: DWI now adds value for both ycMRF and ycEMVI after treatment, the old guideline said it wasn’t accurate for these.
Nodes get read against the tumor. The mesorectal cutoff returns to 5 mm short axis, but don’t be rigid. When the lumen shows a complete response the nodes almost always followed, only about 7% of complete luminal responders have residual nodal disease, and isolated nodal regrowth during watch-and-wait is rare, about 3 to 6% of all local regrowths. For a borderline node in a watch-and-wait candidate, use the test of time, re-image in 6 to 12 weeks. Lateral nodes have no reliable size threshold for restaging, just describe the change and correlate.
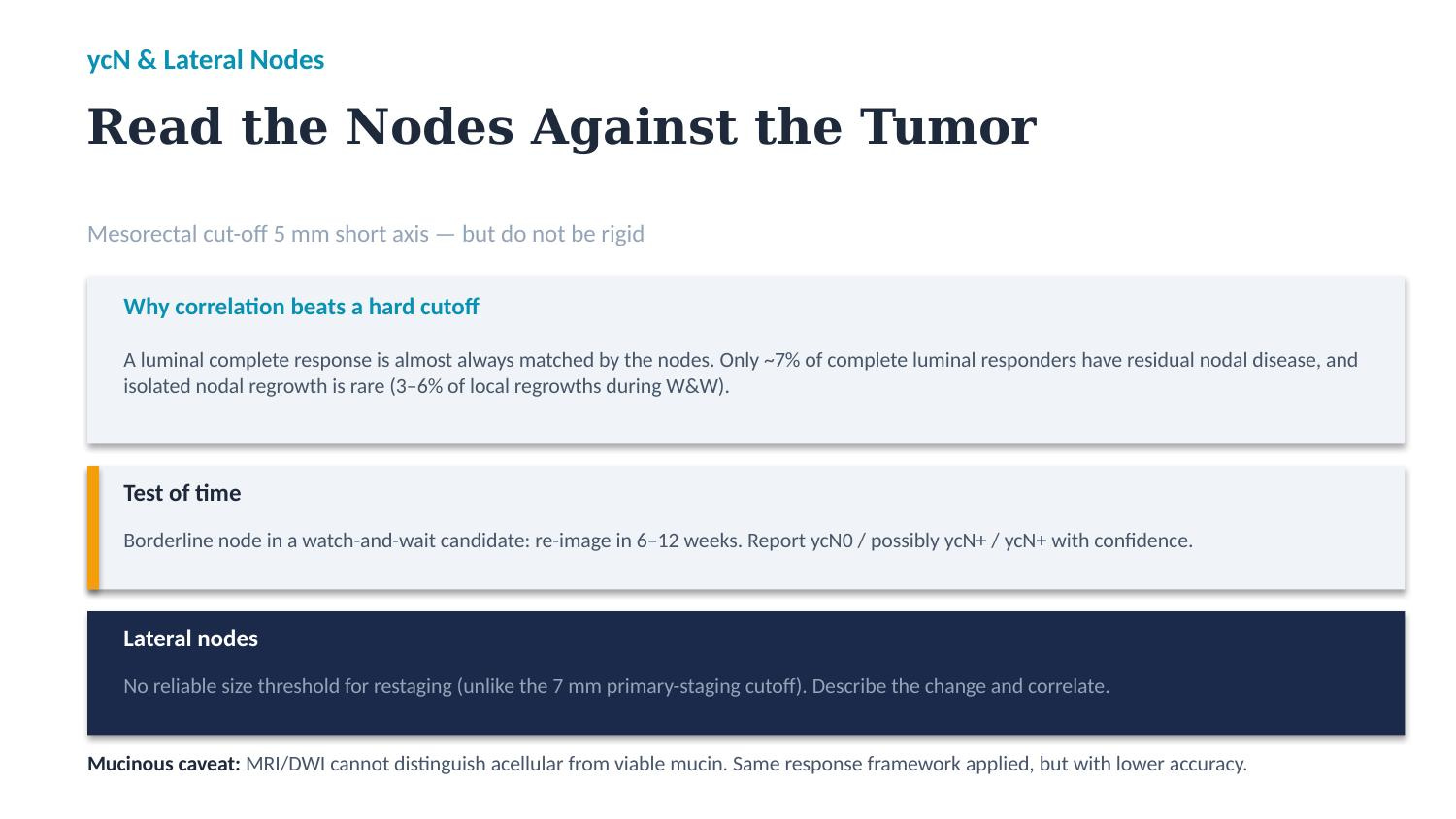
Mucinous tumors are the soft spot. MRI, including DWI, can’t tell acellular mucin (post-treatment, no live cells) from mucin that still contains viable tumor. The flip side, some solid tumors develop mucinous degeneration after chemoradiation, which is just acellular mucin and not a worse tumor. The panel kept the same response framework for mucinous lesions but flagged the lower accuracy. This was the one item that didn’t reach consensus.
What I’d put in the report
The point is to put the response bucket and your confidence in plain language so the team can act on it. Adjust to your style.
Complete response: “Findings compatible with complete response. Homogeneous T2 fibrosis at the prior tumor site, no diffusion restriction, no suspicious mesorectal nodes. ycMRF negative, ycEMVI negative. Suitable for consideration of watch-and-wait, pending endoscopic confirmation.”
Minor residual: “Near-complete response. Small focus of intermediate T2 signal with corresponding restricted diffusion within the fibrotic bed, ycT maximum estimate T2. Mesorectal node at 6 mm short axis without clear regression, ycN possibly positive. Local treatment options could be considered.”
Major residual: “Major residual tumor. Persistent solid mass with diffusion restriction, ycT3b, ycMRF clear at 4 mm. ycEMVI positive grade 4. Three suspicious mesorectal nodes, ycN positive. Findings favor radical surgery.”
Where I’d stay cautious
A few things to hold lightly. The ycT recommendation reads as European practice, US workflows often don’t restage the primary at all. The mucinous response criteria are inherited, not validated, so factor that into your confidence. And MRI lags histology, a near-CR that still has some signal can still be a CR, that’s why short-interval reassessment is in the algorithm.
The bigger picture
Complete response is becoming the goal, not an accident. More of your restaging reads are really one question asked under uncertainty, can this patient safely keep their rectum. Stating that judgment clearly, with your confidence attached, is the job.
That closes the two-part ESGAR update.
Deeper reading
ESGAR 2026 guidelines: Part II, restaging and response evaluation, and Part I, primary staging. Both in European Radiology 2026.
Background on organ preservation: Renehan et al, the OnCoRe project, Lancet Oncology 2016. van der Valk et al, the International Watch and Wait Database, Lancet 2018. Lambregts et al, DWI for selection of complete responders, Annals of Surgical Oncology 2011.