AI in Radiology: What I'm Reading This Month
First in a new monthly RadBrief digest. The papers I read closely this month, and the ones I set aside.
There’s a lot of AI radiology literature each month. I’m trying to figure out what actually changes the work. This is the first AI digest in RadBrief, a new monthly format alongside the abdominal episodes. Two papers I read closely. Two I set aside.
Prefer to watch? The video above is a 3.5-minute deep dive on the featured paper. The two quick hits and the set-aside list below are Substack only.
Featured: AI assist that actually changes what a radiologist decides
Yuan et al. npj Digital Medicine, 2025.
Open access: https://www.nature.com/articles/s41746-025-01970-y
Multicenter CT model for stratifying pancreatic cystic neoplasms, PCNs. The model, called PCN-AI, was trained on 1,835 patients across 4 centers. Contrast-enhanced CT. 63 quantitative features feeding 4 hierarchical classification tasks. Hierarchical means it doesn’t just give you benign or malignant. It walks the WHO classification: mucinous vs non-mucinous, IPMN vs MCN, precancerous vs malignant.
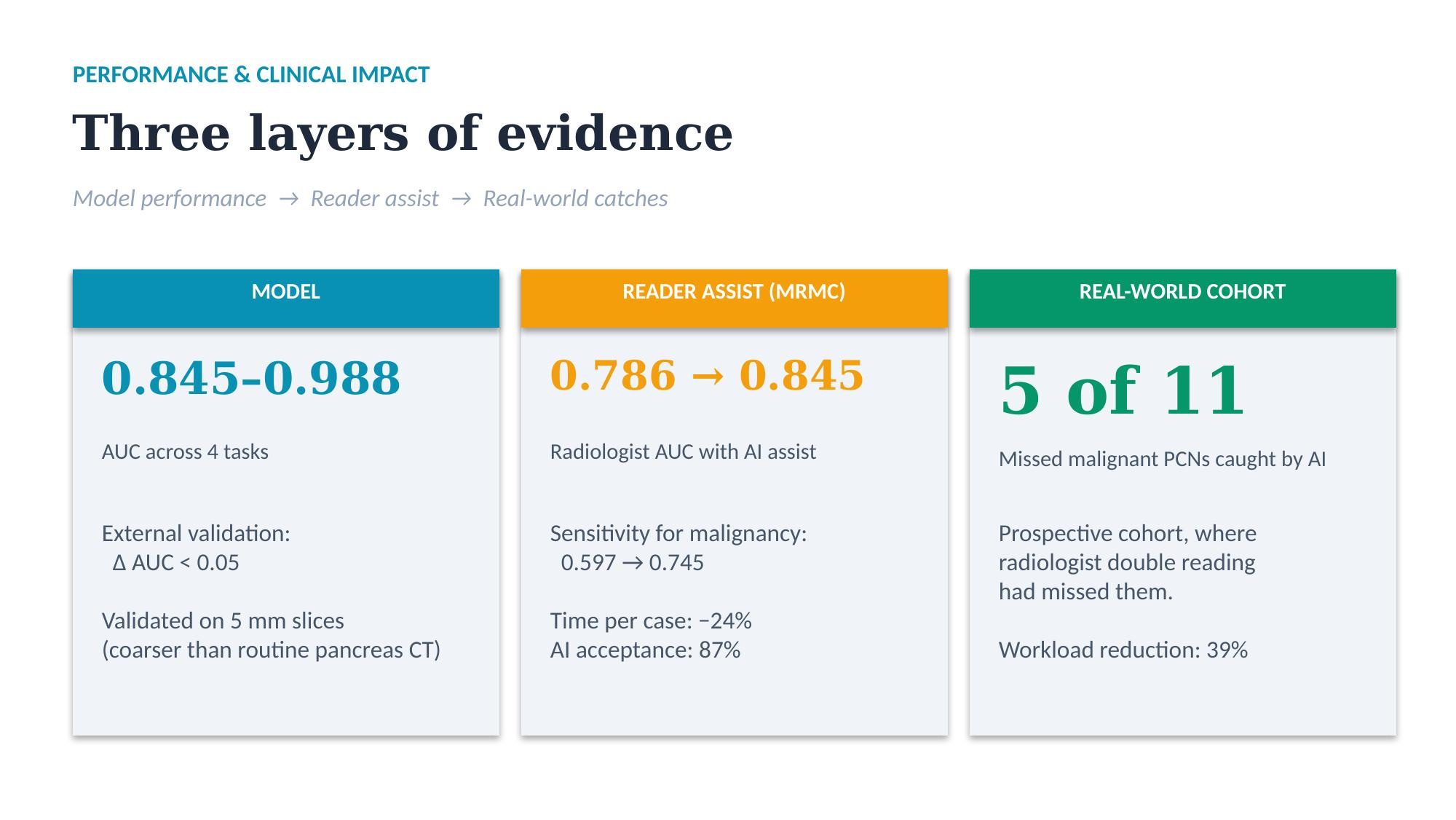
The numbers. AUCs 0.845 to 0.988 across tasks. External validation held up, with delta AUC under 0.05 between internal and external cohorts. Performance was maintained on 5 mm slice CT. That’s thicker than what most centers use for pancreas protocols day to day, where 1 to 3 mm is routine. So they validated on coarser data than our routine, not finer.
The MRMC study. Radiologist accuracy went from AUC 0.786 to 0.845 with AI assist. Sensitivity for malignancy improved from 0.597 to 0.745. Interpretation time dropped 23.7%. Radiologists accepted AI recommendations in 87% of cases.
The prospective real-world cohort. AI flagged 5 of 11 malignant PCNs that radiologist double reading missed, with a 39% workload reduction.
Pancreatic cysts are a hard call. IPMN versus mucinous cystic neoplasm versus serous cystadenoma versus pseudocyst, and the malignancy risk varies across all of them. Most radiologists, including me, hedge in the impression. This is the rare AI paper where the assist actually changes what a radiologist decides, and the prospective real-world arm gives you something stronger than retrospective MRMC alone.
What the abstract doesn’t tell you.
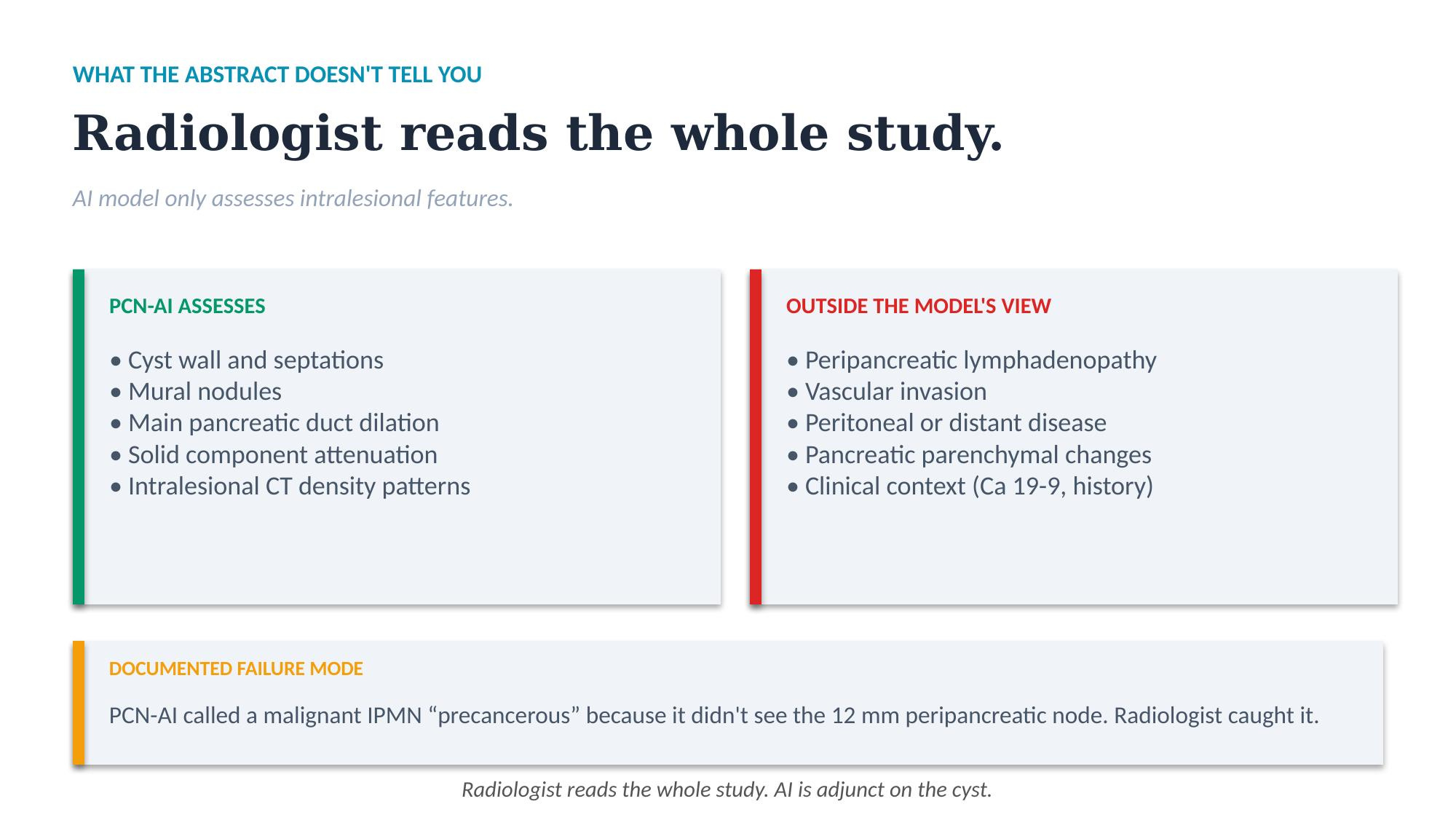
The model only looks at intralesional features. In one documented case, it misclassified a malignant IPMN as precancerous because it didn’t account for a 12 mm peripancreatic lymph node. The radiologist caught it. Treat the tool as adjunct, not a second reader. Peripancreatic context, lymphadenopathy, and vascular invasion sit outside the model’s view. You’re still reading the whole study.
The MRMC has recall bias. Despite randomization and washout, blinded re-reading of a subset showed kappa 0.54, which means the unassisted baseline was probably inflated. The AI improvement is real, but read the numbers with that caveat.
Spectrum bias. They excluded pseudocysts and cystic neuroendocrine tumors, which mimic PCN on CT in practice. So this isn’t AI for any pancreatic cyst. It’s AI for the four PCN subtypes they trained on.
Junior radiologists benefited much more than seniors, delta plus 0.19 vs plus 0.07. I think this is the most interesting subgroup signal in the paper. It tells you who this kind of tool is for: community practices and trainees, more than subspecialty centers.
Leadership angle. If PCN volume is growing in your practice and you want to standardize stratification across readers, this is the strongest evidence base for PCN stratification so far. No FDA-cleared product specifically for PCN stratification exists yet, so this is monitor and pilot, not buy. If your practice is heavy on early-career readers, the case is stronger.
Quick hits
Automated Couinaud segmentation for FLR volumetry. Mathai et al. (NIH and Wisconsin), Radiology: Artificial Intelligence, May 2026. DOI: https://doi.org/10.1148/ryai.250808
3D nnU-Net trained on 498 patients, Medical Segmentation Decathlon plus NIH, tested on 64 internal patients (50 with fibrosis, 8 with PVE) and 247 external patients across colorectal liver mets, cirrhosis, and healthy controls. Whole-liver Dice 0.98 internal and external. FLR Dice 0.99 in the colorectal liver mets dataset. Pre and post-PVE FLR estimates matched the manual reference within 5%, the threshold for agreement on hypertrophy.
Two things make this better than prior Couinaud tools. First, it works on livers with lesions, prior surgery, metal artifacts and embolization coils. Lee et al’s prior tool excluded those patients, and TotalSegmentator wasn’t designed for segment-level Couinaud delineation. Head-to-head on the same external cirrhosis cohort, this model hit Dice 0.91 across Couinaud regions vs 0.79 for Lee et al. Second, the code and training dataset are public.
Code: https://github.com/rsummers11/CT_Couinaud_Segmenter
Bottom line. If you do preop hepatobiliary planning and FLR volumetry, this is the cleanest open-source automated approach to date. Pickhardt and Summers on the author list. Worth tracking what comes out of that group.
Set aside this month
Patient perceptions and attitudes towards AI in a symptomatic breast unit. Singh et al., European Radiology, January 2026. Single-site survey of patient attitudes toward AI in a symptomatic breast clinic. Useful if you’re doing patient communications or designing consent language for AI-assisted screening. Didn’t add anything for me on AI strategy or paper-club discussion.
AI for quantitative assessment of white matter hyperintensities, opportunities and challenges. Li et al., European Radiology, March 2026. Commentary. No new data, no head-to-head results. If I wanted a neuro AI primer, I’d start elsewhere.