The O-RADS score is only as good as the image you put into it.
RadBrief EP07 · The abdominal imaging literature, read for you
▶ Prefer to listen? Hit play above. Same read, about 5 minutes.
O-RADS US works as a gatekeeper. The score decides whether an adnexal lesion gets dismissed, gets a follow-up scan, or gets sent on to MRI, a gynecologist, or surgery. This RadioGraphics review makes a point we tend to skip past: that score is only as reliable as the image it was read from, and US is the one modality where the operator can change the image. So I think the technique isn’t a side note, it’s where the score actually gets decided.
It’s a pictorial review from the ACR O-RADS US committee, the people who wrote the v2022 system, including a Cleveland Clinic author. No new data. What it does is lay out, parameter by parameter, how to acquire and optimize the study so the lexicon works the way it was validated to work. Worth reading alongside the v2022 update itself, which is where the scoring rules and the score table live.
A quick reminder of the stakes. The categories run 0 to 5: 0 technically inadequate, 1 normal ovary, 2 almost certainly benign at under 1 percent risk, 3 low risk at 1 to 10 percent, 4 intermediate at 10 to 50 percent, 5 high at 50 percent or more. The whole point of the system is to keep benign and physiologic lesions out of the OR while not missing the cancers. A technique error that nudges a 2 to a 4, or a 4 down to a 2, lands directly on a patient.
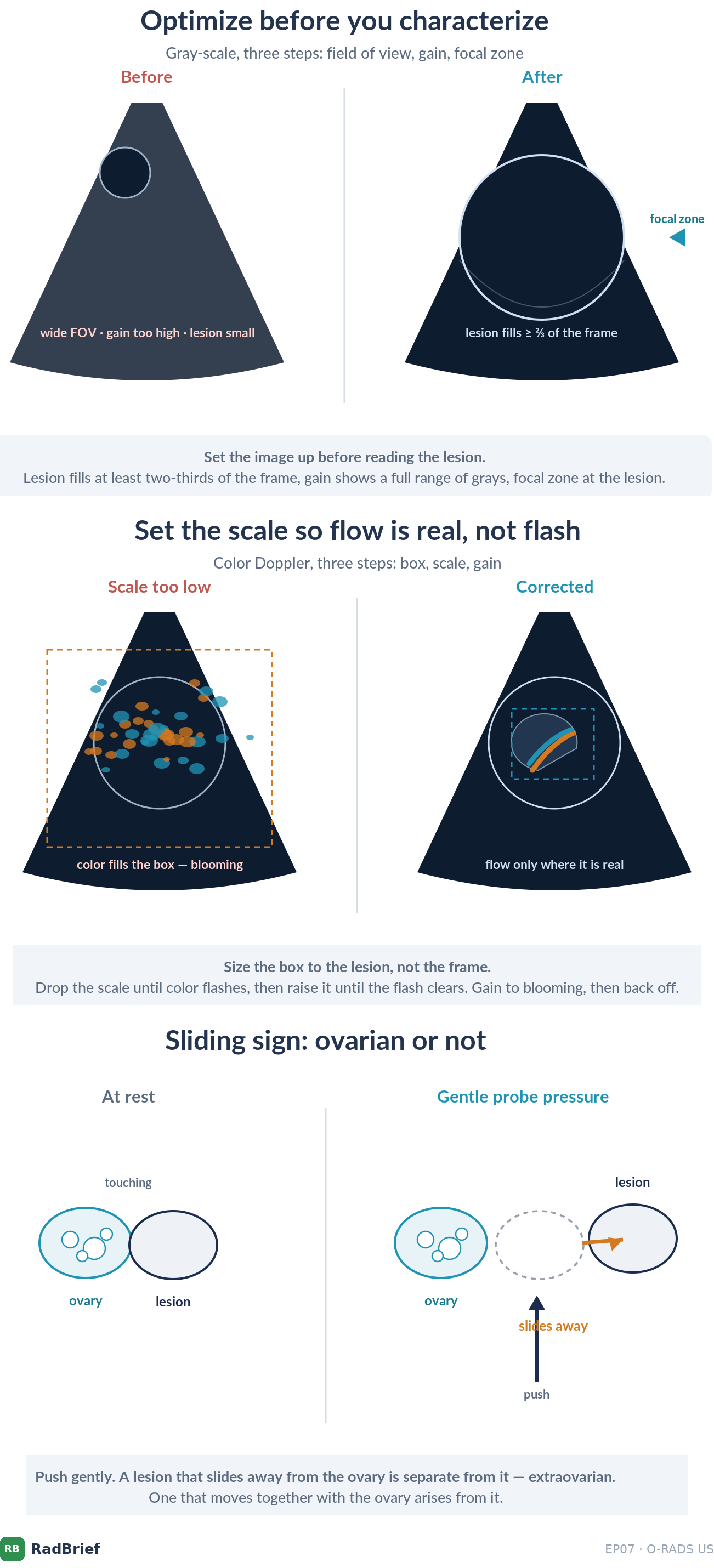
What I’d tell a resident. I’d optimize before characterizing. Gray-scale is a three-step habit: field of view first (set depth to include the whole lesion plus enough tissue behind it to judge posterior shadowing, then narrow the width so the lesion fills at least two-thirds of the screen), then gain (enough to show a full range of grays, using bladder, follicles, and vessels as your internal reference), then focal zone at or just below the lesion. Color Doppler is its own three steps: size the box to the lesion and not the whole frame, or you lose sensitivity for the flow you’re after; drop the scale until color flashes, then raise it until the flash clears; set color gain to blooming, then back it off. The maneuvers matter too, because they change scores, and a resident should know them even though the sonographer is the one holding the probe. The sliding sign sorts ovarian from extraovarian origin, and the jiggle separates mobile debris from a real solid component. Bowel displacement, a hand on the lower abdomen pushing toward the probe tip, rescues an ovary buried behind gas. Knowing these exist is what lets you spot when one was needed and ask for it, and it’s how you avoid an O-RADS 0 or a wrong number.
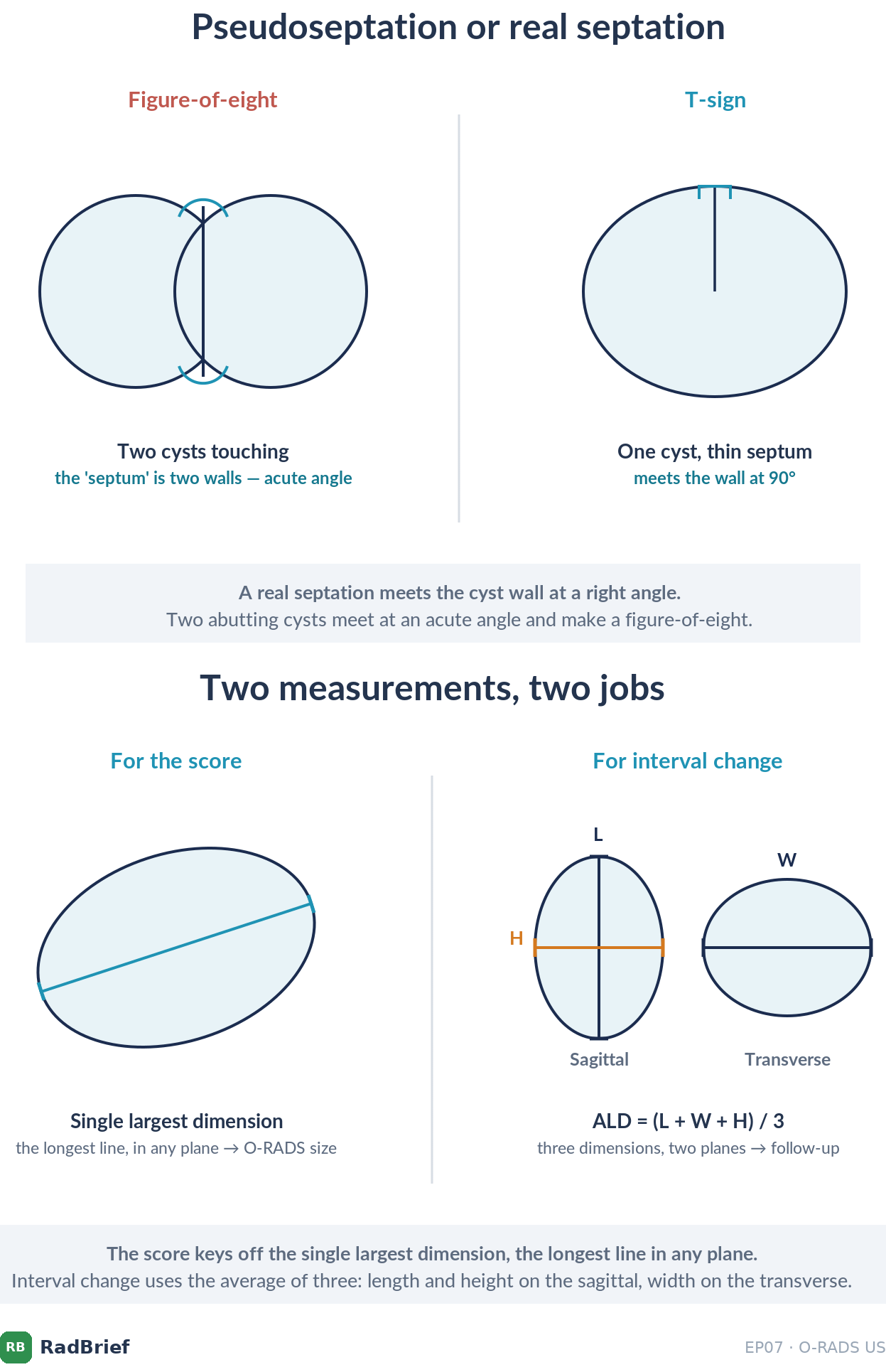
What I’d tell a general radiologist. Most of us aren’t scanning live. We’re reading static images and clips a sonographer acquired, so our job is knowing what can fake a score and not signing off without what we need. The artifacts that matter are the ones that move a lesion between categories. Side-lobe and mirror artifact put echoes inside a simple cyst and make it look solid. Gain set too high turns a simple cyst complex, too low turns a solid lesion cystic. Refractive edge artifact gets misread as shadowing, and shadowing is a benign feature for smooth solid lesions, so calling it wrong can down-score a cancer. Pseudoseptations are everywhere: the figure-of-eight sign of two abutting cysts versus the clean T-sign of a true complete septation, cyst-in-a-cyst from partial volume averaging, the cumulus oophorus. There are two things I’d want before signing. Cine clips in orthogonal planes, because a 3 mm papillary projection or a mobile echo is often invisible on the still frame someone chose to save. And measurement done in real time: the score keys off the single largest dimension in any plane, and interval change off the average linear dimension, length plus width plus height over three. Neither reconstructs honestly from workstation calipers after the fact. If the images don’t let you do that, I think the better call is sometimes to ask for a repeat rather than force a number.
What we should be skeptical about. This is expert guidance, not evidence. There’s no outcome data here showing that optimized technique catches more cancers or sends fewer benign cysts to surgery. It almost certainly does, but the paper codifies good practice rather than proving it. And it names operator dependence without removing it. The whole approach assumes a skilled sonographer, a cooperative transvaginal exam, and a radiologist who can review clips and request maneuvers in real time. Plenty of practices don’t have all three. So I read this as the standard to push toward and a checklist worth handing your sonographers, while being honest that the floor it’s trying to raise is still set by whoever holds the probe.
I’m Melina Pectasides, and this is RadBrief.
Reference block: driving the O-RADS US exam
Screenshot this. Hand it to your sonographers.
Gray-scale, three steps
FOV: depth to include the lesion plus posterior tissue (so you can judge shadowing), then width so the lesion fills ≥ 2/3 of the screen
Gain: full range of grays; calibrate against bladder, follicles, vessels
Focal zone: at or just below the lesion (multiple zones drop the frame rate)
Color Doppler, three steps
Box: sized to the lesion, not the whole frame
Scale: lower until color flashes, then raise until the flash clears
Color gain: raise to blooming, then back off
Maneuvers that change the score
Sliding sign: ovarian vs extraovarian origin
Jiggle: mobile debris vs true solid component (presence of motion is informative; absence is not)
Bowel displacement: hand on the hemipelvis toward the probe tip
Wait for peristalsis: bowel mimicking a dermoid
Don’t get fooled
Side-lobe / mirror artifact faking a solid component in a simple cyst
Refractive edge artifact misread as shadowing (risks down-scoring a smooth solid lesion)
Pseudoseptation (figure-of-eight) vs true septation (T-sign)
Gain too high makes cysts look solid; too low makes solids look cystic
Measurement
Score off the single largest dimension, any plane, found in real time by turning the probe
Interval change off ALD = (length + width + height) / 3, better for deformable cysts
Solid component = projects ≥ 3 mm into the lumen; < 3 mm is wall/septal irregularity
Spectral Doppler confirms true flow but does not feed the risk score
Deeper reading
Underlying data: the IOTA (International Ovarian Tumor Analysis) studies, which the O-RADS lexicon’s malignancy estimates are built on. [confirm exact citation + DOI before publishing]
Companion to EP02 and EP03, the ESGAR rectal MRI pair, in the same “how the system actually gets applied” register.