Perianal Fistula MRI: The Report Is the New Frontier
How I Do It, twenty years on: the technique question is closed, and the report is the new frontier.
RadBrief Episode 05 — Companion post. Catch up on prior episodes at joinradbrief.com.
Stoker and Halligan wrote the State of the Art on perianal fistula imaging in 2006. Twenty years later, same journal, same two authors, a How I Do It. I think the contrast is the most useful thing about it. The technique conversation is basically over. The weight has moved to two things: how you report the fistula, and how you assess response after treatment.
So this post is built around the report, not the protocol. The protocol matters and I’ll cover it, but it’s not where the last twenty years went.
Start with what the surgeon actually wants. Two answers. What is the relationship between the fistula and the sphincter, can it be laid open without making the patient incontinent. And are there any extensions that will cause recurrence, and where. That’s it. Most reports don’t lead with those two things. The 2026 paper is trying to fix that.
Anatomy, fast. The sphincter is 4 to 5 cm. Inside out: mucosa, internal sphincter, the intersphincteric space with its longitudinal layer, then the external sphincter, with puborectalis taking over in the upper half. The dentate line sits roughly mid-canal. You won’t see it directly, but you can estimate it, and coronal helps. About twelve anal glands sit around it, and their infection is where most cryptoglandular fistulas start. That’s the whole reason the intersphincteric plane matters so much.
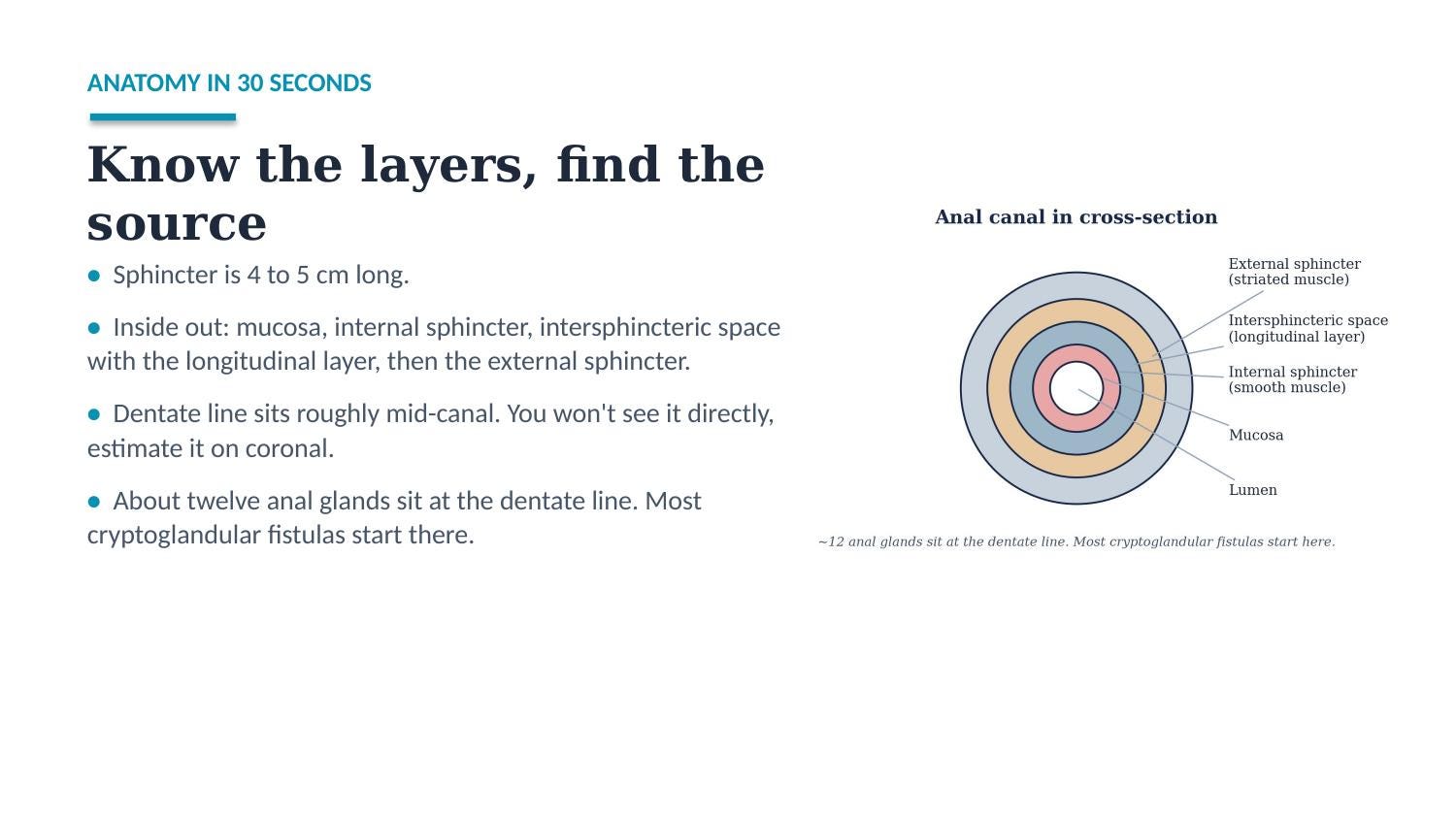
The layers, inside out. Most cryptoglandular fistulas start at the anal glands around the dentate line.
Parks still holds. Intersphincteric, transsphincteric, suprasphincteric, extrasphincteric. The first three start as intersphincteric infection. The fourth comes from higher up, so if you see extrasphincteric disease, look at the rectum.
Get the obliques right or the rest is wrong. Three planes, aligned to the anal canal axis, not the body axis. Plan from the sagittal scout, coronal parallel to the canal, axial orthogonal to it. This is the single most common technical error I see on outside studies. If the obliques drift, the classification drifts with them. T2 without fat-sat for anatomy, T2 with fat-sat or STIR for active tracts and abscesses, and IV contrast only if you need it, it’s optional and there’s no consensus. Two don’ts the paper is explicit about: no diffusion, it lacks the resolution for subtle findings, and don’t run an enterography protocol for a fistula question, it’s inadequate for the sphincter. Coverage is the quiet failure point, the axial obliques need the full sphincter, the anorectal junction, and a few sections above, or you miss supralevator disease.
Now the report, which is the point. Lead with the two surgical questions. Everything else is supporting evidence. The paper anchors its reporting section in the ESGAR minimum dataset, and there’s one line worth taping to the workstation.
“Radiologists must use language that surgeons understand.”
— Stoker & Halligan, Radiology 2026
The minimum dataset is six items. The clinical question. The fistula, with its radial location, Parks class, and openings. Any extensions, with location and maximal diameter. Sphincter integrity. Associated findings. And comparison with prior. Six items, that’s the entire ask. Most reports either skip three of them or bury them under two paragraphs of descriptive prose about twists and turns the surgeon will never use. If you want the six items at the workstation without hunting, RadReason’s Ask feature pulls up the ESGAR dataset on command.
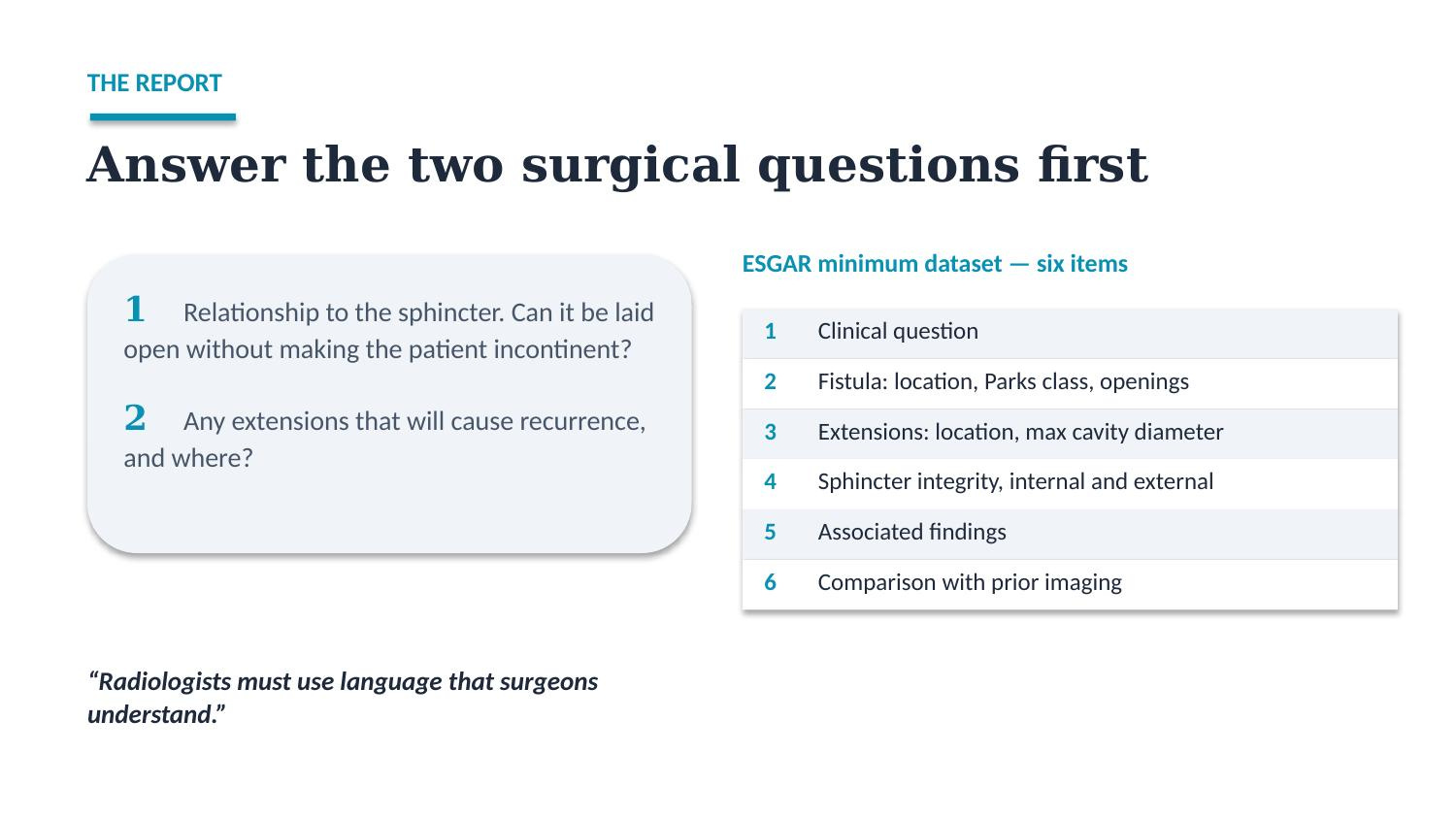
Answer the two surgical questions first. The six-item ESGAR dataset is the rest of the report.
Response and healing is the genuinely new part. This is what 2006 didn’t have. For trials there’s the MAGNIFI-CD score, accurate but too slow for daily work. For daily practice, use the TOpClass consensus: treatment response is increased fibrosis, a clear drop in tract diameter, length, or abscess size, and loss of the bright T2 signal. A healed fistula is a fully fibrotic tract, no bright fat-sat T2 signal, no enhancement if you gave contrast. Re-image somewhere around 3 to 6 months after treatment starts.
Then apply that strictly. Subtle residual abnormality predicts recurrence. The paper shows a case where a faint curvilinear hyperintensity was called healed, and the patient came back clinically a year later. When you’re calling healing, a second look at the fat-sat T2 is worth the thirty seconds.
Don’t get fooled. Two mimics worth knowing. Pilonidal sinus, midline and posterior and subcutaneous, rarely crosses the intersphincteric plane or has an internal opening, and that absence is the diagnostic key. Hidradenitis suppurativa, extensive and superficial, apocrine glands, spares the sphincter, but can coexist with Crohn’s and muddy the read. And think Crohn’s even without a diagnosis when you see extrasphincteric disease, a watering-can anus, multiple extensions, or skin involvement. The surgeon may not have called it yet. Suggest it.
Malignant transformation is rare, but the cost of missing it is high. Suspect it with deterioration after many years, mucoid or bloodstained discharge, a new mass-like lobulation, or a budding appearance. Most cases won’t look like cancer. The ones that do, look again.
What I’d put in the report
The point is to answer the two questions in language the surgeon can act on, then the dataset. Adjust to your style.
Simple transsphincteric: “Single transsphincteric fistula, internal opening at 6 o’clock at the dentate line, external opening in the left posterior perineum. Tract crosses the lower third of the external sphincter. No extension, no abscess. Sphincters otherwise intact. Amenable to consideration of fistulotomy with low continence risk.”
Complex, likely Crohn’s: “Multiple intersphincteric tracts (watering-can pattern) with a transsphincteric component on the right, internal opening at 5 o’clock. Right supralevator extension, maximal cavity 3 cm, with a seton in situ. Findings raise the possibility of Crohn’s disease. Not suitable for simple fistulotomy.”
Post-treatment, healed: “Compared with [prior], the previously active transsphincteric tract is now a thin fibrotic band with no hyperintense fat-sat T2 signal and no enhancement. Findings compatible with a healed fistula. No new tract or collection.”
Where I’d stay cautious
A few things to hold lightly. The optimal post-treatment imaging interval isn’t settled, 3 to 6 months is reasoned, not proven. The internal opening is often never widely patent, so don’t invent a location you can’t trace, report the most likely site as the point of maximal intersphincteric infection. And healing on MRI lags the clinical picture in both directions, which is exactly why you apply the criteria strictly and re-look when it’s borderline.
The bigger picture
Twenty years closed the technique question and opened the reporting one. More of the value now sits in saying the two things the surgeon needs, clearly, and in being honest about healing when the signal is subtle. That’s a reasoning problem, not an imaging one, and it’s the kind of judgment I built RadReason to support.
Watch the full episode: RadBrief EP05 on YouTube (paste the episode URL here at publish).
Deeper reading
The two papers this episode is built on.
How I Do It: MRI Approach to Perianal Fistulas. Stoker J, Halligan S. Radiology 2026.
Imaging of fistula in ano. Halligan S, Stoker J. Radiology 2006.
Foundational and consensus references behind the recommendations.
ESGAR consensus on imaging of fistula-in-ano. Halligan S, Tolan D, Amitai MM, et al. European Radiology 2020.
Defining radiological healing in perianal fistulizing Crohn’s disease (TOpClass Delphi consensus). Anand E, Devi J, Ballard DH, et al. Clinical Gastroenterology and Hepatology 2025.
Buchanan GN, Halligan S, Williams AB, et al. “Effect of MRI on clinical outcome of recurrent fistula-in-ano.” Lancet 2002. The study that made perianal MRI routine, 16% recurrence when surgeons acted on it versus 57% when they didn’t.