One in four LI-RADS 3 lesions doesn't stay a 3
RadBrief EP09 · The abdominal imaging literature, read for you
Prefer to listen? Hit play above. Same read, about 4 minutes.
A LI-RADS 3 is the score we tend to set aside. It means indeterminate, so we say repeat in three to six months and move on. This paper is the largest cohort so far on what actually happens to those lesions, and the main finding is that about one in four does not stay a 3. At one year, 28 percent of LI-RADS 3 observations had moved up: 14 percent to LI-RADS 4, 14 percent to LI-RADS 5. So indeterminate is not the same as low risk, and I think that changes how seriously we read the next follow-up.
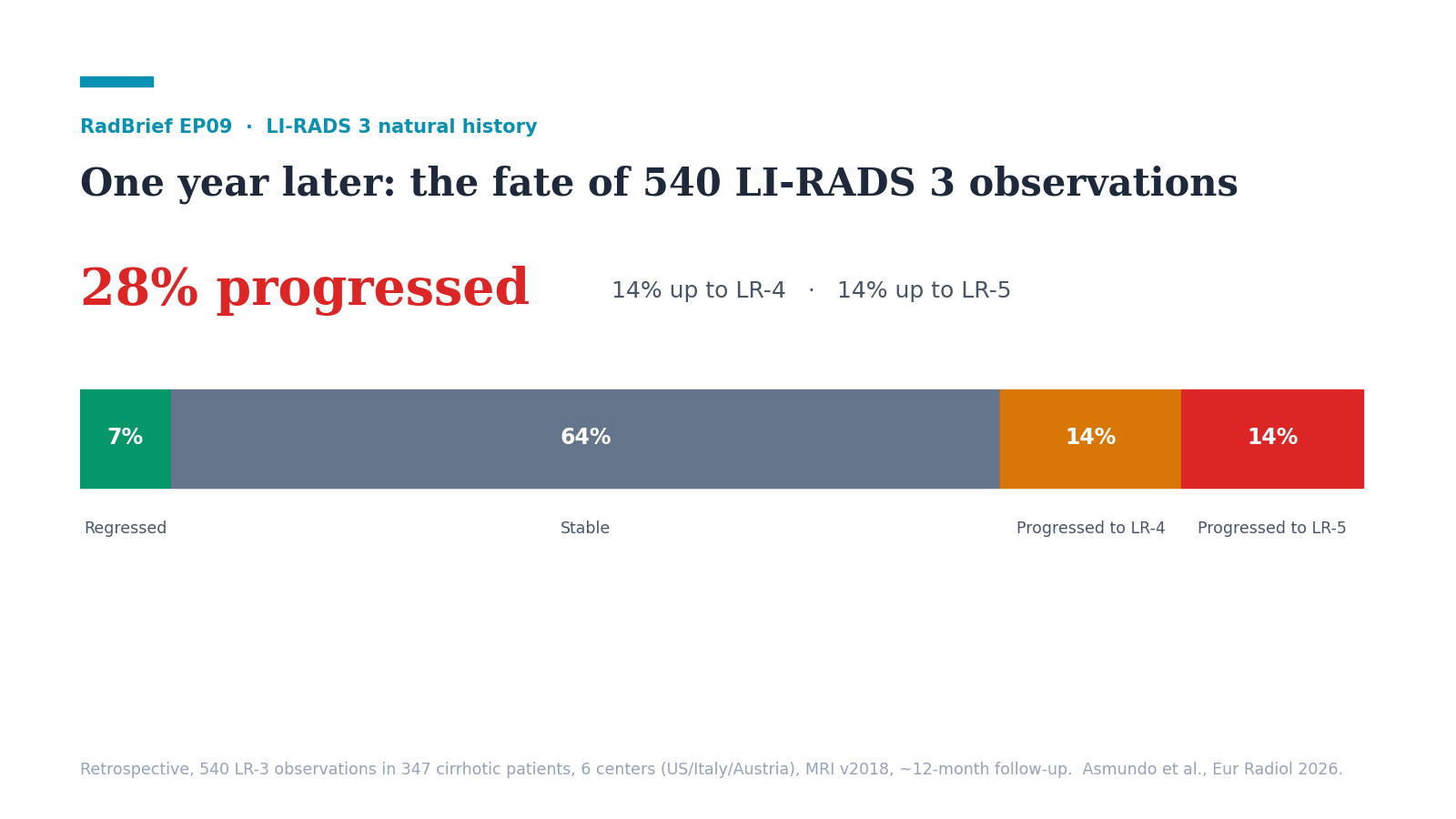
It’s a retrospective study of 540 LI-RADS 3 observations in 347 cirrhotic patients across six centers in the US, Italy, and Austria, all re-read on MRI with v2018 criteria and all with a follow-up scan at twelve months, plus or minus three. There’s no histopathology, so progression here means the imaging category changed, not that anyone biopsied a cancer. What it adds over the older single-center work is size and consistency. Prior single-center studies put overall LR-3 progression somewhere in the 12 to 20 percent range, and this reports 28 percent with a cleaner design, and it identifies which lesions are more likely to progress.
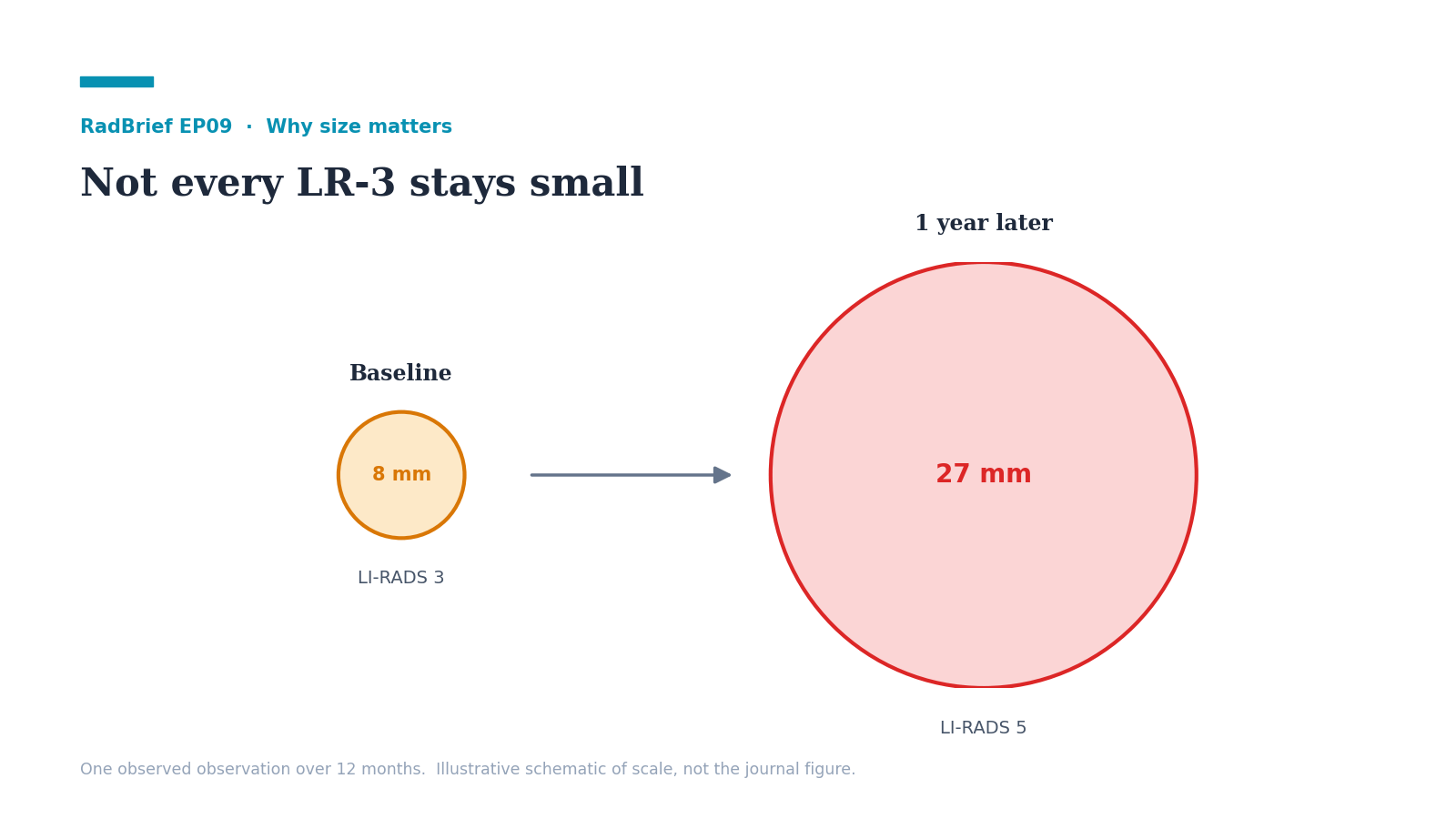
What I’d tell a resident. The number to hold is one in four, and that it splits evenly, 14 percent up to a 4 and 14 percent up to a 5. LR-3 is not “probably nothing.” The single most useful predictor is size. Each additional millimeter raised the odds of progression by about 12 percent, and the lesions that moved up were generally larger, with a threshold landing around 9.5 millimeters. But I’d hold that cutoff loosely, because on its own it was only 58 percent sensitive and 63 percent specific, so it points toward closer attention, not a rule you’d act on. And none of this changes what LR-3 already tells you to do, which is repeat imaging in three to six months. The paper tells you which of those follow-ups you’d watch harder, not that you’d stop following the rest.
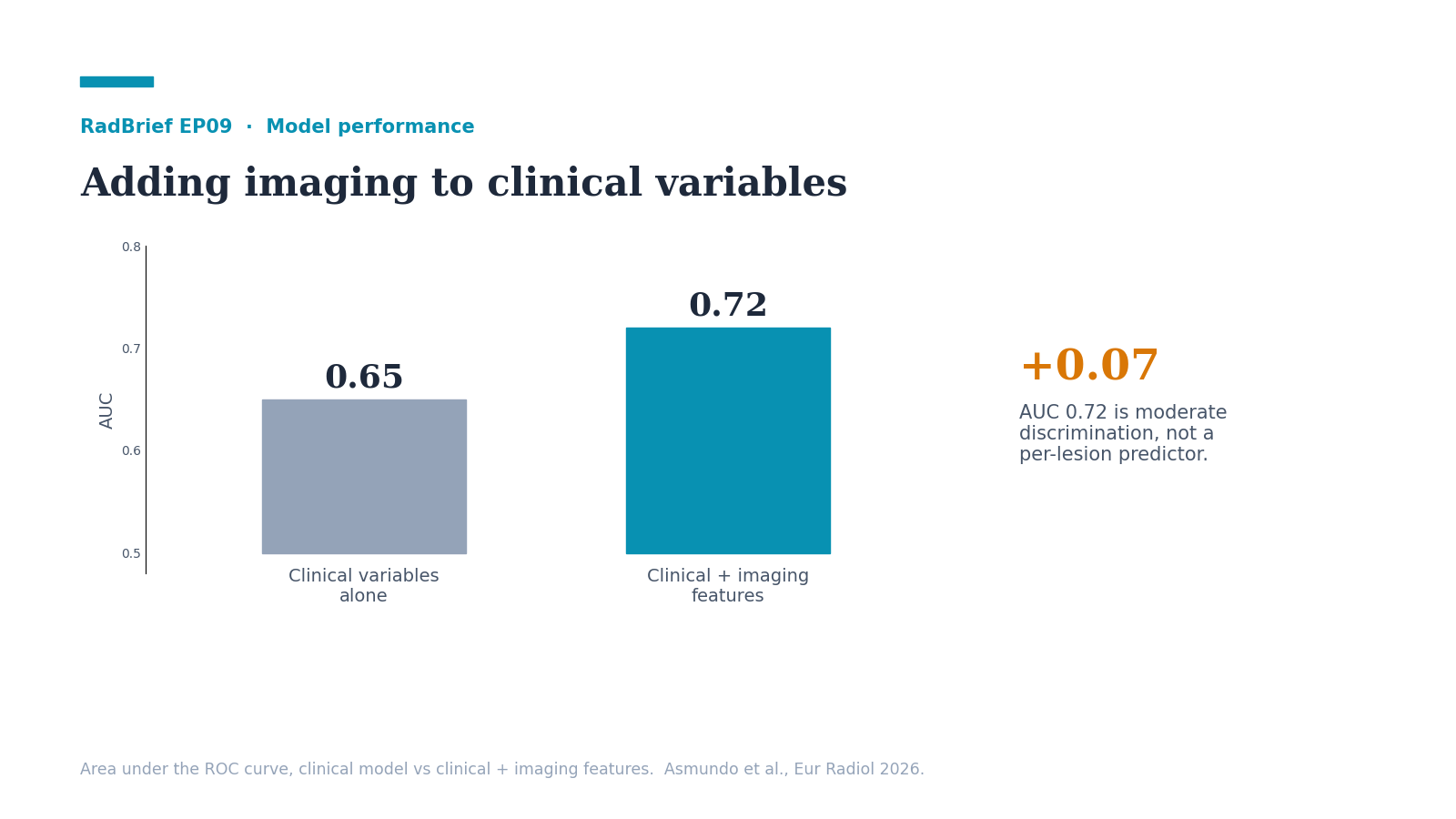
What I’d tell a general radiologist. The useful change is to stop treating every LR-3 the same. Three things marked the higher-risk ones: larger size, worse liver function at Child-Pugh C, and, on univariable analysis, untreated hepatitis C and a coexistent LI-RADS 5 elsewhere in the same liver. Alcohol-related cirrhosis actually went the other way and was associated with lower progression, probably because those livers develop regenerative and hyperplastic nodules that sit at LR-3 and stay there. Clinical context mattered too: a model with clinical variables alone reached an AUC of 0.65, and adding the imaging features moved it to 0.72. So an LR-3 in a decompensated cirrhotic with a growing sub-centimeter nodule is not the same lesion as an LR-3 in a treated-HCV Child A liver, even though both get the same number on the report. I’d size it carefully in real time and note any coexistent LR-4 or 5, because those are the flags the next reader can act on.
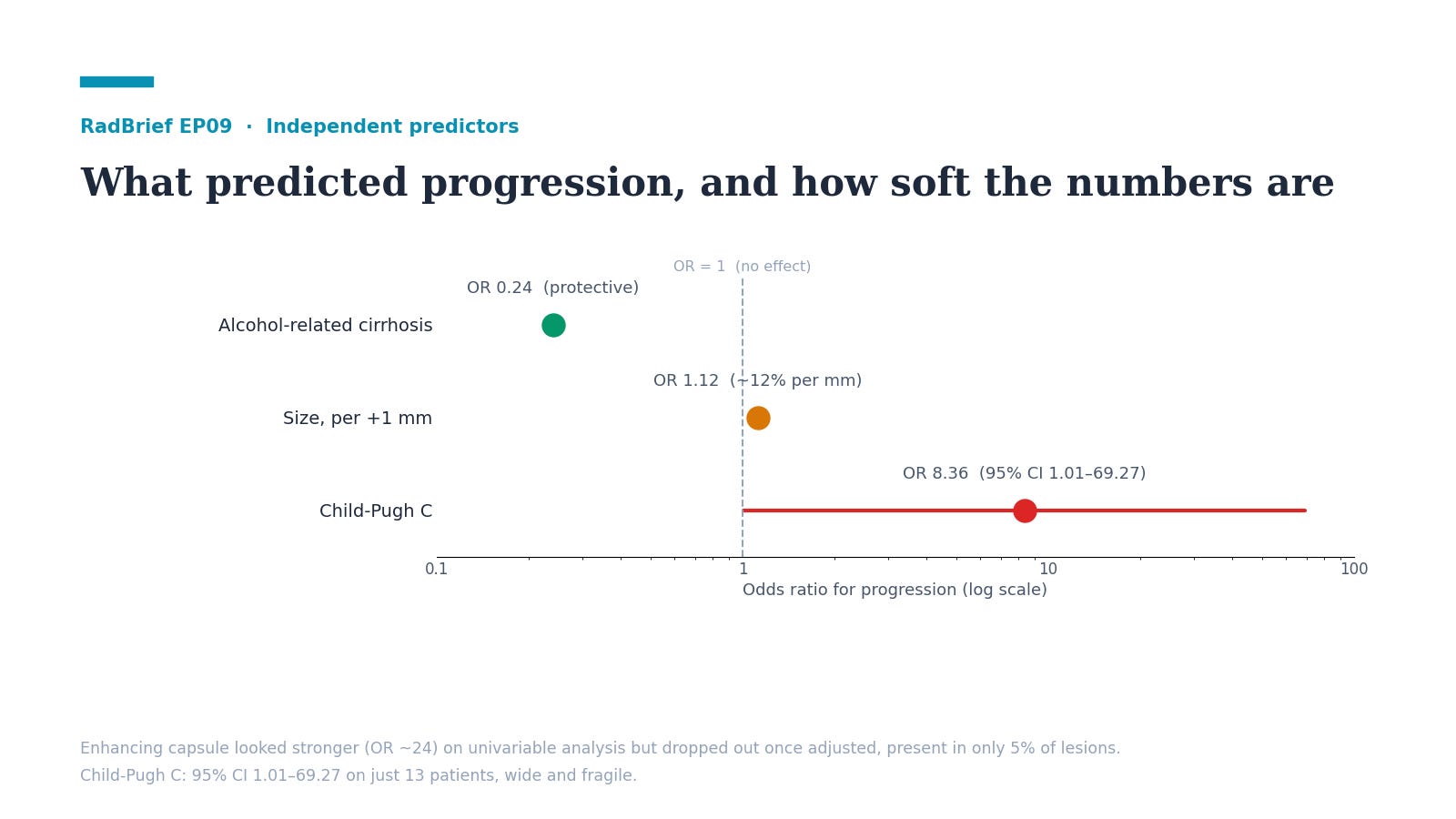
What we should be skeptical about. The predictors are softer than they look. Child-Pugh C came out with an odds ratio of 8.36, which sounds dramatic until you see the confidence interval, 1.01 to 69.27, off only 13 Child C patients and barely significant at p equals 0.049. I wouldn’t read too much into the size of that number. The enhancing capsule looked even stronger on univariable analysis, an odds ratio near 24, but it appeared in only 5 percent of lesions and dropped out once the model adjusted for everything else. The deeper issue is the outcome itself. Progression means the imaging category changed, so the study is partly measuring one imaging read against a later imaging read rather than against tissue. And because they only included patients who came back for a clean twelve-month MRI, the ones treated early or lost to follow-up are gone, which most likely undercounts the true progression rate. The combined model reaches an AUC of 0.72, which is moderate. So I read this as good calibration for how seriously to take an LR-3, not a per-lesion predictor I’d act on by itself.
I’m Melina Pectasides, and this is RadBrief.